Introduction
Mental health is a fundamental aspect of human well-being and is defined as the state in which individuals are aware of their own capacities, able to cope with stress in daily life, work productively, and contribute to the community (WHO, 2013). Mental health can be affected by a variety of biological, social, and environmental factors (WHO, 2013). Among the social factors are issues of discrimination and violence, as is the case for individuals with diverse sexual orientations or gender identities (Meyer, 1995, 2003). One variety of this discrimination and violence is homophobia. Homophobia is defined as hatred, fear or aversion towards lesbian, gay, bisexual, and transgender people (henceforward referred to as LGBT) (Herek, 2004; UNESCO, 2015).
Homophobia can be expressed as discrimination and/or violence. In turn, discrimination can be understood as any act or omission based on gender, ethnicity or sexual orientation that obstructs or undermines a person’s access to human rights and liberties (Official Gazette, 2016). Violence can also be expressed in acts or omissions that cause an individual physical, psychological or sexual harm or suffering (INMUJERES, 2009).
Homophobia has social roots in three aspects of the gender system. Firstly, hetero-sexism, understood as an ideological system that considers heterosexuality to be the only sexual norm and orientation (Herek, 2004). This ideology is inextricably linked to the alleged human need to reproduce that only categorizes people as male or female (Warner, 1993; Wittig, 2005). Secondly, the fulfillment of gender stereotypes, or a collection of beliefs about how men and women should behave (Rocha & Díaz-Loving, 2011), derived from a binary gender perspective or the hegemonic norm of socializing according to rules regulating femininity if the person is a woman and masculinity if the person is a man (Ortíz-Hernández, 2005; Castañeda, 2006). Lastly, there is andro-centrism, which places men and masculinity above women and femininity (Castañeda, 2006; Lagarde, 1997; Ortíz-Hernández, 2005). Expressions of homophobia include internalized homophobia (IH): the LGBT person’s own acceptance of the negative premises and beliefs surrounding sexual diversity (Ortíz-Hernández, 2005; Ross & Rosser, 1996).
The literature suggests that LBGT people are usually more affected by depression, anxiety, and alcohol and drug use (Cochran & Mays, 2006; Russell, 2006) than heterosexuals (Almeida et al., 2009; Mustanski, Garofolo & Emerson, 2010), They also suffer from distress rooted in the discrimination, violence, and stigma they experience (Herek & Garnets, 2007; Meyer, 1995; Meyer, 2003; Ortíz-Hernández, 2005), for which internalized homophobia is one of the main risk factors. In Mexico, high IH levels are linked to suicide attempts and ideation, mental disorders, and alcoholism (Granados-Cosme, Torres-Cruz & Delgado-Sánchez, 2009). Nevertheless, there are no data linking IH to depressive symptomatology or alcohol consumption.
Other data from Mexican studies show that alcohol use is more frequent amongst the LGBT community and that two of the primary motivators of alcohol abuse are discrimination and homophobic violence (Espolea, 2015; Mendoza, Ortíz & Román, 2016). Data show that nearly 90% of gay men and lesbian women consume alcohol (8% of gay men and 5% of lesbians drink alcohol at least twice a week). This type of information indicates that, despite the discrimination and violence experienced by the LGBT population sharing the same social roots, behavior relevant to mental health differs between the subgroups of this population. This is due to the different ways in which each group transgresses gender stereotypes (Ortíz-Hernández, 2005). For example, gay men and transgender people clearly violate the norms established by gender and masculinity systems. Despite existing recognition and support of human rights for LGBT people in Mexico, this community is still exposed to a hostile social environment. Between 66.9% and 83.6% of LGBT people report having experienced discrimination based on their sexual orientation or gender identity (Lozano-Verduzco & Salinas-Quiroz, 2016; Mendoza, Ortíz & Román, 2016).
Literature from the United States on the issue identifies minority stress and community connectedness (CC) as two variables associated with social homophobia and the subjective conflicts experienced by LGBT people (Frost & Meyer, 2012; Meyer, 2003). Community connectedness indicates how close an individual feels to other LGBT people. Efforts to study the state of health of the Mexican LGBT community have been limited, except for sexual health and HIV issues (Bautista, Colchero, Sosa, Romero & Conde, 2012).
It is important to design studies to understand how the LGBT community is both discriminated against and violated, and how this connects with its mental health. Bearing this in mind, this article seeks to link internalized homophobia, community connectedness, violence, and discrimination to two primary mental health indicators: alcohol use (AU) and depressive symptomatology (DS). IH, discrimination, and violence are expected to be positively linked (directly proportional) to AU and DS; and CC, to be negatively associated (inversely proportional) to AU and DS. Furthermore, the strength of each association is expected to vary according to the group being studied (gay, lesbian, bisexual, and transgender people).
Method
Study design and selection procedure
A cross sectional analytical study was undertaken to estimate how the perception of discrimination is associated with violence (physical, sexual or emotional) and how IH and CC are associated with the presence of DS and AU among LGBT people in Mexico City. Participants in the study were chosen through purposive sampling. The two criteria for inclusion were: to identify as LGBT and to live in Mexico City.
The questionnaire was applied in two different ways. The first form of application entailed inviting participants of the Sexual Diversity and Pride Parade in Mexico City in June 2015 to answer the questionnaire face to face. Undergraduate volunteers from the Psychology Department of the National Pedagogic University were trained for the endeavor. The volunteers followed the instruction to invite all participants to answer all questions. The second was to upload the same questionnaire to the virtual platform Monkey (Waclauski, 2012). This platform does not allow participants to advance through the questionnaire until they have answered each question. The virtual survey was spread through various digital social networks with the help of civil organizations and governmental bodies between June 27 and August 7, 2015. Our descriptive analysis of the sample showed no important differences in sociodemographic characteristics (age, socioeconomic level or educational attainment) between those who answered the questionnaire at the Parade and those who answered it online.
Study sample: We personally applied 793 questionnaires at the Parade and another 3 087 were answered online, for a total of 3880. Of the total, 556 participants were identified as heterosexual and four did not specify any sexual orientation; 474 reported they did not live in Mexico City, reducing our analytic sample for analysis to 2 846 participants.
Measuring tools and operationalization of the variables
IH: The IH scale was adapted for the Mexican population (Lozano-Verduzco & Salinas-Quiroz, 2016; Ortíz-Hernández, 2005), including 14 questions with Likert scale answer values between 1 and 5. Reliability for this scale was .874, with an explained variance of 57.85%. The questions were designed to reveal the desire of no longer wanting to be LGBT, efforts to change one’s sexual orientation, and a preference of living as heterosexual.
CC: This section was adapted and validated for this particular study (Frost & Meyer, 2012; Lozano-Verduzco & Salinas-Quiroz, 2016). It included eight questions to be answered on a Likert-type scale of five options grouped as a single factor with a reliability rate of 0.896 and an explained variance of 58.7%. Questions were designed to indicate how deeply connected to the LGBT community individuals were, and how close they felt to other people like them.
DS: We used the General Health Questionnaire validated by university students (Romero & Medina-Mora, 1987) and used with LGBT sample groups (Ortíz-Hernández, 2005). It included twelve questions, ten of which were answered on a 5-option Likert scale, one on a 4-option Likert scale and two on a dichotomous scale, making a total score of 58. The score was divided into terciles. The questions were designed to highlight symptoms of depression, suicide attempts or ideation, and feelings of happiness or sadness.
Discrimination (Brito et al., 2012): This section included 15 questions to be answered dichotomously; they were designed to explore where the respondents experienced discrimination and who perpetrated it. The questions were built upon the definition of discrimination of the Consejo Nacional para Prevenir y Eliminar la Discriminación (National Council on Discrimination Prevention and Elimination) (Ley Federal para Prevenir y Eliminar la Discriminación, 2016). Questions were coded no=1 and yes=2, allowing for scores between 16 and 30 to identify the presence of discrimination and 15 to indicate no discrimination.
Violence (Brito et al., 2012): This section included seven dichotomous questions exploring various violent behaviors from the victim’s perspective. The maximum score was 14 points (“yes” answers coded as 2 points and “no” answers coded as 1 point). Scores of 8-14 indicated that the subject had been a victim of violence in at least one of the areas evaluated. The items asked whether the respondent had been a victim of physical, emotional or sexual violence by actors such as neighbors, relatives or police officers.
AU: Alcohol use was evaluated through six questions taken from the Alcohol Use Disorder Identification Test (AUDIT) (Babor, Higgins-Biddle, Sasunders & Monterio, 2001; Ortíz-Hernández, 2005). The questions were answered on a Likert scale with five answer choices (0-4), with a final total of 24 points, one the frequency and amount of drinks, feelings of guilt about drinking, and others.
Sociodemographic co-variables: Civil status, classified into two categories: steady partner and no partner; educational attainment: categorized by level and whether the person completed the level or not, summarized in nine categories.
Socioeconomic level: The section, based on the scale proposed by the Mexican Market Intelligence and Opinion Association (AMAI), included eight variables. There were seven categories (AB, C+, C, C-; D+, D, E); for the purpose of regression analysis, the socioeconomic levels were grouped into three categories (upper, middle, and lower; AB for upper, C+-D for middle, and E for lower). Upper level indicates the possibility of acquiring luxuries such as holidays outside the country and new cars; middle level indicates the possibility of acquiring the basic basket and a few luxuries; and lower level indicates difficulty in purchasing even basic items.
Statistical analysis
We carried out a descriptive analysis of the variables according to the LGBT group each subject belonged to. Chi-square type proportion comparison tests were done for the categorical variables, while the differences in the questionnaire scores between groups were evaluated through the Kruskal-Wallis test.
We also analyzed the association between IH, CC, violence, and discrimination and the presence of AU and DS. Evaluations of the distribution of AC and DS scores within each study group demonstrated over-dispersion (variance > mean), given that in all the tests: the dispersion index (VT), proof of Chi-square goodness-of-fit, and the asymptotic test O2, the null hypothesis of equidispersion was consistently rejected (p < .05). Accordingly, it was decided to use a negative binomial regression analysis for each answer (AU and DS) for each group. In all the adjusted models, the over-dispersion alpha parameter was shown to be statistically different from zero, and the verisimilitude ratio test demonstrated a significant improvement in each adjusted model with respect to its corresponding Poisson version. All the assumptions in the model were verified, including the distribution of Pearson, Anscombe and deviance generalized residuals.
By means of a sub-analysis, the results were compared by the type of measurement of the variables (in-person or online), with no differences being found in the models’ betas. This was done by making multiplicative interaction terms for each of the betas with the “type of questionnaire” variable, and in no case were these terms of interaction significant. We used STATA/IC®, version 12.1. software to carry out our analyses.
Ethical considerations
The project protocol was approved by the research committee at the Universidad Pedagógica Nacional. Steps were taken to ensure that all respondents gave their informed consent before participating in the survey and agreed that their answers would be used for research purposes. The information was analyzed anonymously and no names or identifying features were recorded for any of the participants, thereby guaranteeing confidentiality.
Results
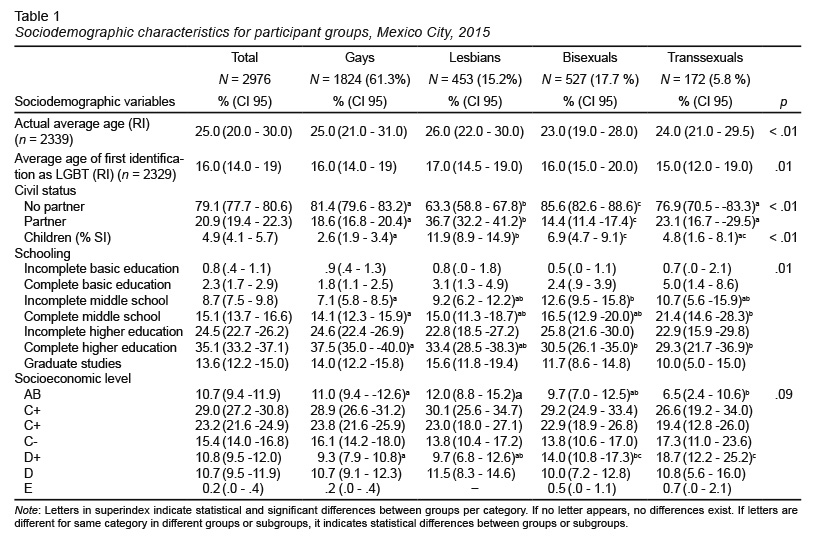
The analytical sample included 2 846 participants ages 13 to 70; of these, 61.3% were identified as gay, 15.2% as lesbians, 17.7% as bisexuals, and 5.8% as transsexual. Table 1 shows the distribution of primary sociodemographic characteristics among the participants as a whole and for LGBT subgroups.
Adjusted associations between social determinants for DS and AU
Table 2 and Table 3 show the results of the binomial regression models for AU and DS scores. Given the differences between the LGBT groups, models were created for each group as well as a consolidated model, adjusting the DS, violence, CC, and socioeconomic level scores by tercile.
In the consolidated model for AU, positive associations were observed with levels of discrimination, violence, and CC. Having an average discrimination score –with respect to a low score– β = .06, 95% CI [.01, .11], and a high score for violence, compared to a low score β = .09, 95% CI [.02, .16] and an average score for CC –as compared to a high level– increases AU scores (β = .11, 95%: CI [.06, 0.17]) (Table 2).
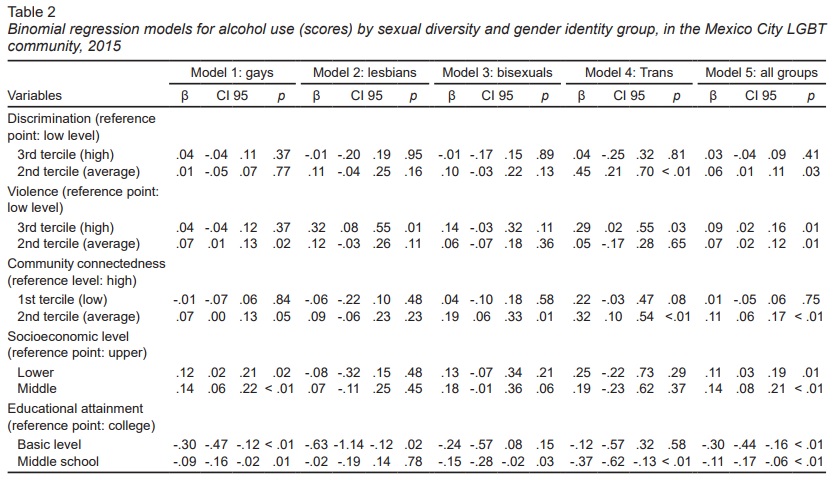
When AU was analyzed for LGBT groups, it was positively associated with an average level of violence as opposed to a low level. β = .07, 95% CI [.01, .13], having a lower or middle socioeconomic level versus an upper level. β = .12, 95% CI [.02, .21] for lower socioeconomic level and β = .14, 95% CI [.06, .22] for medium socioeconomic levels among gay men.
For the lesbian group, AU was positively associated with high levels of violence as opposed to low levels. β = .32, 95% CI [.08, .55]. In the bisexual group, an average CC –as compared to a high CC– increased the likelihood of AU (β = .19, 95% CI [.06, .33]). In the transsexual group, AU was positively associated with an average discrimination score (β = .45, 95% CI [.21, .70]) and an average CC score (β = .32, 95% CI [.10, .54]) (Table 2).
In the consolidated model for the presence of DS, we observed positive associations with the levels of violence and CC. Having an average or high violence score –with respect to a low violence score– increased the possibility of having DS (β = .12, 95% CI [.06, .18] for an average level of violence; β = .13, 95% CI [.05, .21] for a high level of violence).
Having an average or high CC score –with respect to a low CC score– increased the possibility of having DS (β = .16, 95% CI[.09, .23] for a low level of CC; β = .13, 95% CI [.06, .19] for a high level of CC) (Table 3).
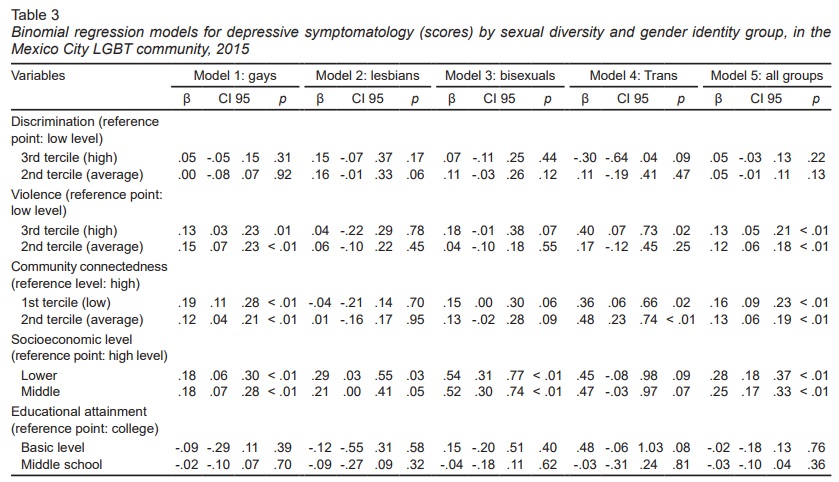
An analysis of the presence of SD for LGBT groups showed that among gay men, this variable is positively associated with an average and high level of violence, –compared to a low level of violence– (β = .15, 95% CI [.07, .23] for an average level of violence; β = .13, 95% CI [.03, .23] for high levels of violence).
Low and average CC levels increased the possibilities of depressive symptomatology in the group of gay men. β = .19, 95% CI [.11, .28] for low CC; β = .12, 95% CI [.04, .21] for average CC). Among the groups of lesbians and bisexuals, no notable variables were associated with DS (Table 3).
Among the group of transsexuals, a positive association was observed between DS scores, violence levels, and CC. This model was the most similar to the consolidated model. Having a high violence score (β = .40, 95% CI [.07, .73]) and a low or average CC score (β = .36; 95% CI [.06, .66] for low CC; β = .48; 95% CI [.23, .74] for average CC) was associated with high levels of DS.
Discussion and conclusion
This data indicates that as hypothesized, violence and discrimination impact on aspects of mental health. Specifically, high and average levels of violence were positively associated with both DS and AU and average levels of discrimination were positively associated with AU, both of which indicate that the greater the violence experienced by victims, the more likely they are to display DS and AU. Discrimination was associated differently since medium levels of discrimination are associated with aspects of mental health. This may be due to the fact that since discrimination is more subtly expressed than violence, it may be more difficult for the victim to identify it.
Data also showed that average levels of CC were associated with high levels of AU and DS. This may be due to high CC scores acting as mental health protectors. Likewise, people with low CC scores may not qualify as part of the LGBT community, thereby reducing their identification with victimization as a result of homophobic discrimination and violence. For both discrimination and CC, the data behave in a curvilinear manner, where the extremes for both variables indicated weaker connections with mental health and average scores indicated a stronger association.
Both DS and AU may lead to greater health issues such as illegal substance abuse, liver disease, depression, and suicidal ideation (Babor et al., 2001). Structural interventions are therefore important preventive measures, as in the case of the fight against discrimination, particularly in health care systems, but also in other areas where homophobia is prevalent, such as families and schools (Mendoza, Ortíz & Román, 2016).
These data show that two aspects of mental health (DS and AU) are significantly related to forms of violence rooted in a chauvinistic, homophobic culture. These health problems could be prevented by reducing homophobia and encouraging the flexibilization of the gender stereotypes that give rise to these forms of discrimination and violence. Likewise, empowering the LGBT community and making these identities more visible is another strategy that could improve the mental health conditions of this community.
There are a number of legal provisions and regulations in Mexico that recognize equal rights for LGBT members. Furthermore, there are institutions with the specific purpose of fighting against discrimination based on sexual orientation and gender identity. Nevertheless, society’s respect for and acceptance of sexual diversity is advancing at a different rhythm. The eradication of homophobia would have a positive impact not only on the exercise of human rights, but also on the physical and mental health of LGBT people.
This data are an initial approach to understanding how homophobic expressions are related to certain elements of mental health and should be considered within their limitations. Specifically, the sample is taken from Mexico City, where both LGBT visibility and homophobia are more evident than in other parts of the country. Our analysis did not cover other forms of non-heterosexual identification such as “queer” and “pansexual.” Although these tend to appear to a lesser degree, they may display different relations with the variables of interest. Lastly, it was impossible to control whether or not the same person answered the online questionnaire several times, leading to possible biases in the results.