Introduction
Suicide is a multifactorial phenomenon, whose main determinants include biological, sociocultural, economic, familial, and intrapersonal aspects, chronic-degenerative diseases, and mental disorders (WHO, 2018a). It is currently recognized as a public health problem that is the third leading cause of death in the population aged 15 to 44 worldwide (Bachmann, 2018).
In 2016, the World Health Organization (WHO) reported a global suicide rate of 10.6 per 100,000 inhabitants, 7.7 in women and 13.5 in men, representing approximately 800,000 suicides per year, with one suicide estimated to occur every 40 seconds (WHO, 2018a).
A 275% rise in the prevalence of suicide was reported from 1970 to 2007 in Mexico, which has seen a linear increase in suicide rates since 1984 (Borges, Orozco, Benjet, & Medina-Mora, 2010). Between 2000 and 2013, 64,298 suicide cases were registered in Mexico, where the rate increased in both sexes, from 5.95 to 8.12 in men and from 1.06 to 1.73 in women, with a male-to-female ratio of 4.5:1 (Fernández-Niño et al., 2016). The most recent data published by the Instituto Nacional de Estadística y Geografía [National Institute of Statistic and Geography] indicated a national rate of 5.1 per 100,000 inhabitants (INEGI, 2018).
This increase in suicide rates has been accompanied by the seasonal factor, with the highest suicide rates being found in the summer months (Swade & Coppen, 1980). A non-systematic review observed a significant seasonal effect in suicide rates in various studies undertaken in different countries, where suicides peaked in the spring and summer months (Ajdacic-Gross, Bopp, Ring, Gutzwiller, & Rossler, 2010). A recent study in Mexico found that from 2000 to 2013 May was the month with the highest number of suicides, while February had the lowest number in both sexes (Fernández-Niño et al., 2016).
Various studies based on analyses of Poisson regression models have estimated the increase in suicide in relation to environmental temperature. In England and Wales, after a one-degree temperature rise above 18°C, suicide risk increased from 3.8% to 5.0% (Page, Hajat, & Kovats, 2007), while in South Korea, high temperatures were associated with a relative risk of an increase in the number of suicides (Kalkstein, Belorid, Dixon, Kim, & Bremer, 2019).
In addition, as has been reported in the literature, environmental temperature is associated with thermal stress, a higher risk of infectious diseases, and an increase in natural disasters such as floods or, conversely, droughts and forest fires (McMichael, Woodruff, & Hales, 2006).
Chihuahua is one of the states in Mexico that has registered higher temperatures during the summer months in recent years (CONAGUA, 2020). In addition, it is a subtropical region, 73% of which has a dry or “semi-dry” climate.
In 2016, Chihuahua had the highest suicide rate nationwide, with 11.4 per 100,000 inhabitants. Recent data from the Encuesta Nacional de Consumo de Drogas, Alcohol y Tabaco [National Survey of Dryg, Alcohol and Tobacco Use] indicate that during that same year it also displayed the highest prevalence of suicide attempts in the country (Borges et al., 2019). The objectives of the present study were therefore to analyze the seasonal behavior of completed suicides in the state of Chihuahua and the trend in suicide rates by sex and age group between 2008 and 2018 to generate updated information that will make it possible to implement more effective prevention strategies in the future.
Method
This study was undertaken with data on deaths by suicide obtained from statistics from the Instituto Nacional de Estadística y Geografía [INEGI, 2001; National Institute of Statistic and Geography] (INEGI, 2001) between 2008 and 2018 in the state of Chihuahua. The death registration process is completed when a death certificate is completed and issued by the civil registry office. In the time covered by this study, 3,572 records of completed suicide were presented. Data collection involved obtaining the number of intentional self-inflicted injuries through an examination of the detailed causes of the ICD-10 (X605 to X849) in the accidental and violent deaths section of mortality rates.
Moreover, variables such as the month and year of occurrence, sex, and age were obtained, which were classified into seven age groups in keeping with other similar studies (Shah, 2012; Shah & Coupe, 2009):10-24, 25-34, 35-44, 45-54, 55-64, 65-74 and 75 or over, educational attainment, suicide method, marital status, being an indigenous language speaker, urban or rural residence and economic activity, and whether the person who committed suicide was employed. Data on being an indigenous language speaker, economic activity, and suicide method are available as of 2012. For the remaining variables, data are available from 2008 onwards.
This study also considered the daily average temperature record by weather station, which in turn was averaged per month to be used as a covariate regarding the number of suicides. Temperature data were obtained from the Servicio Meteorológico Nacional [National Meteorological Service] from the statistical climate information database.
Statistical analysis
Suicide rates standardized by sex and age group were calculated for each of the months and years of study for every 100,000 inhabitants, based on population projections by the Consejo Nacional de Población [CONAPO, National Population Council] using the 2005 and 2010 population censuses.
In the categorical variables such as age group, sex, educational attainment, marital status, being an indigenous language speaker, economic activity, and suicide method, a multivariate correspondence analysis was performed. Previously, the relationship of these variables was analyzed through a simple correspondence analysis where the p value of chi squared ≤ .05 was considered a significant relationship.
Since data on being an indigenous language speaker and suicide method are only available as of 2012, multiple correspondence analyses were undertaken on the years when only some of the variables were available.
A univariate analysis of time series was carried out in which the suicide trend from 2008 to 2018 and the Ljung-Box test were determined to establish the self-correlation of observations in that period. The seasonality factor expressed as a percentage and the Dickey-Fuller test were used to establish the seasonality of the observations. In addition, a Poisson regression model was performed to establish the association between temperature and the number of suicides by sex. Lastly, to analyze the relationship between the suicide rate and age groups, Spearman’s rho coefficient was determined, as suggested in other studies (Shah, 2007; Shah & Coupe, 2009), and a time series and linear regression analysis was undertaken to analyze the possible increase in the suicide rate in each of the age groups.
All tests were performed with a 95% confidence interval.
Ethical considerations
This study is based on the INEGI Terms of Free Use of Information.
Results
During the period from 2008 to 2018, a total of 3,572 suicides occurred in the state of Chihuahua, 80% of which corresponded to men and 20% to women. The years with the highest suicide rates were 2015 (11.7), 2016 (12.0), and 2017 (11.1), with 422, 439, and 410 completed suicides, respectively.
Regarding educational attainment, 68% of those who committed suicide had completed high school or less. As for marital status, 34% were single, 25% married, and 18% were partnered, while the most common suicide method was poisoning with 71% and firearms with 14%. Table 1 shows the remaining socioeconomic variables from 2008 to 2018.
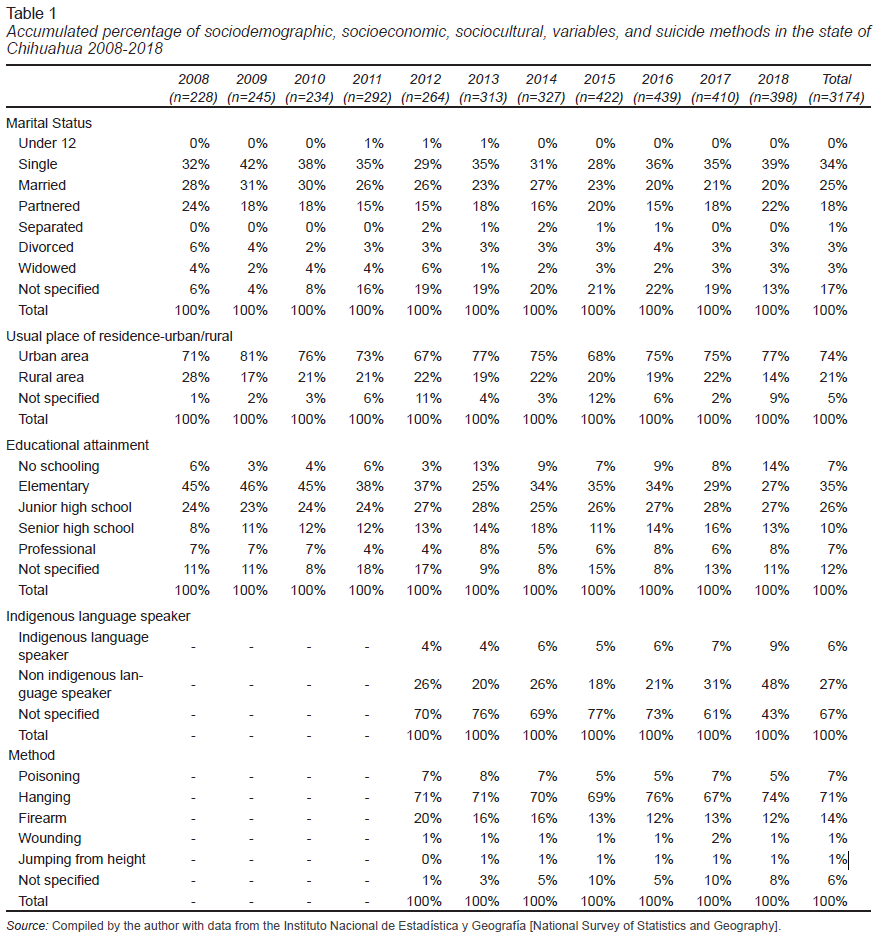
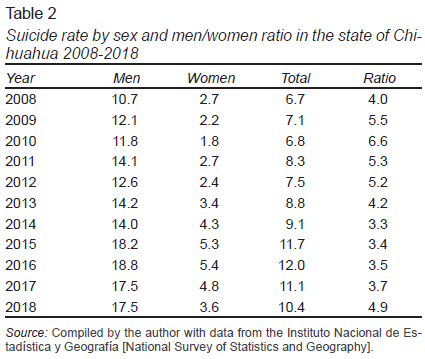
Regarding gender, a suicide rate of 14.5 in men and 3.5 in women was found during the period studied, with a male-to-female ratio of suicides of 4:1 (Table 2).
A multiple correspondence analysis was performed between the variables of sex, age group, marital status, and suicide method with 2,568 valid cases (between 2012 and 2018), which comprised two dimensions, accounting for 77.5% of the variance. Figure 1a shows a link between the categories of people ages 10 to 24 and 25 to 34 and the suspension/hanging and jumping from a height method (the former being associated more with men and the latter with women). A second association between categories was found between married and divorced people ages 35 to 44 and 45 to 54 and wounding and poisoning, mainly in women, while a third was found between the use of firearms and men over 65.
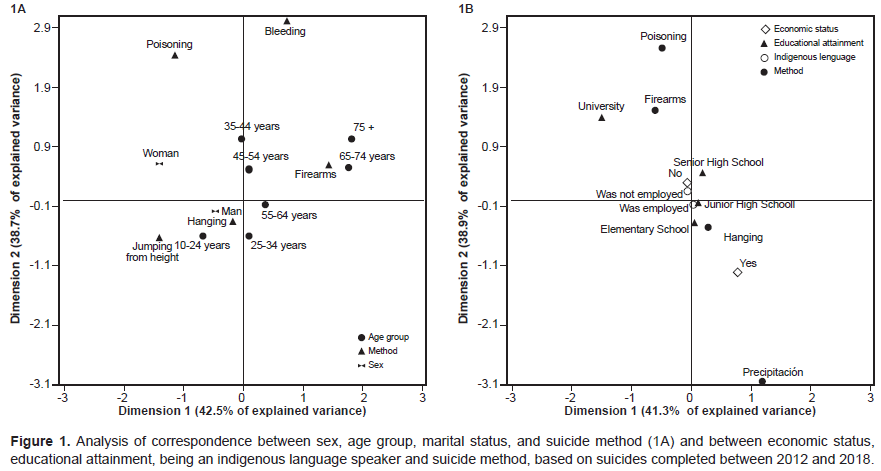
A second analysis of multiple correspondence between being an indigenous language speaker, economic status, educational attainment, and suicide method explained 80.2% of the variance and revealed the association between committing suicide by jumping from height, being an indigenous language speaker, and only having completed elementary school. A second association was observed between people with a university degree and committing suicide using firearms or poisoning (Figure 1b).
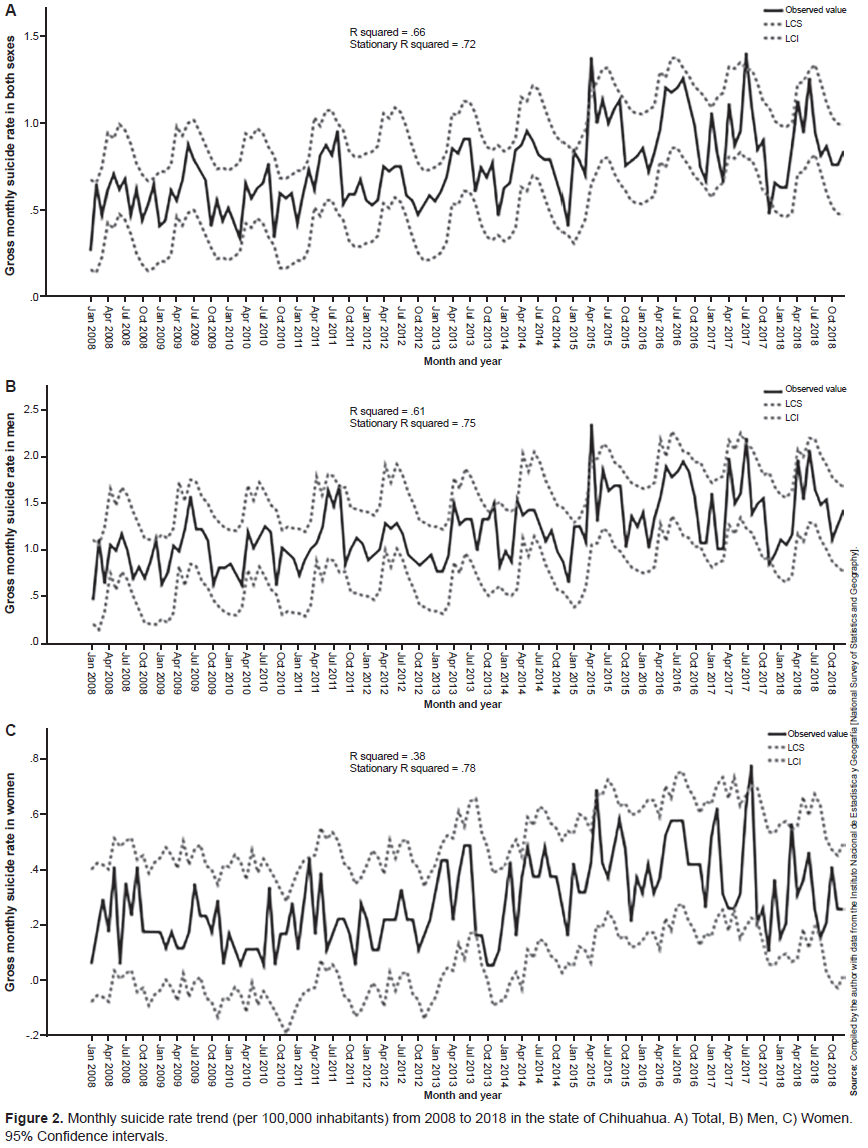
The time series analysis revealed a trend in the increase in suicide rates from 2008 to 2018 in men and women, both separately and together, with a stationary R2 of .75, .78, and .72, respectively (p < .01); graphs are shown in Figure 2 . Moreover, according to the Box-Ljung test, randomness and independence of data were observed for the models of men and for the study universe (p > .43).
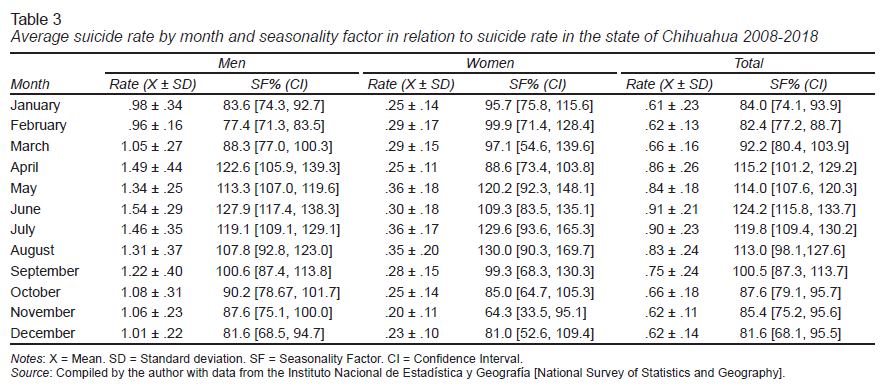
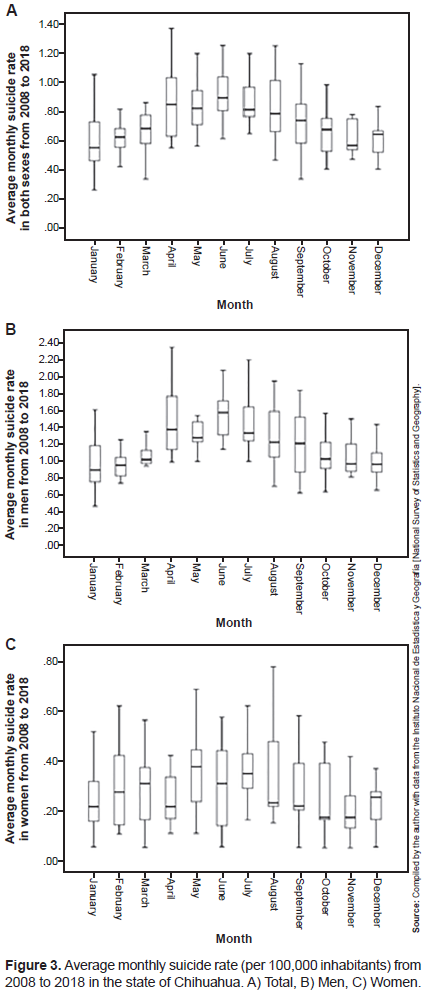
Likewise, based on the Dickey-Fuller test, seasonality was observed in the suicide rate (p = .002 in men, p = .001 in women, and p = .009 overall). Table 3 shows the percentage of the seasonality factor by sex, where the highest suicide rate in men according to the seasonality factor occurred in the months of April, June, and July, when it increased by 13%, 28%, and 19%, respectively. Conversely, suicide rates in women increased in May, July, and August by 20%, 30% and 30%, respectively. For the two sexes combined, it increased by 24% in June and 20% in July. Figure 3 shows the diagram of the seasonality factor for each sex and the two combined.
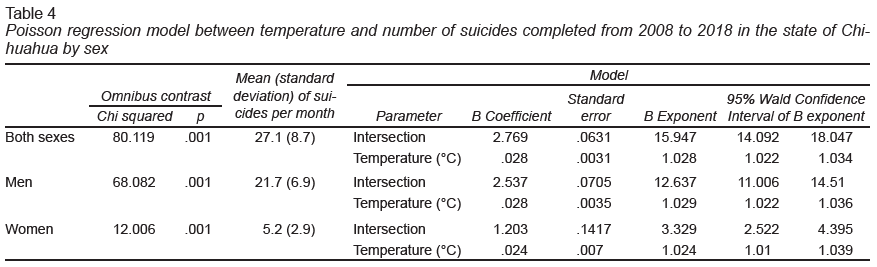
An analysis of the effect of temperature on the number of suicides in the two sexes combined through an analysis with a Poisson regression model revealed an association between temperature and the number of suicides from 2008 to 2018. For every one-degree Celsius increase, the risk of suicide rose by 1,028 in the two sexes combined, with 1,029 in men and 1,024 in women. Table 4 provides a summary of the model.
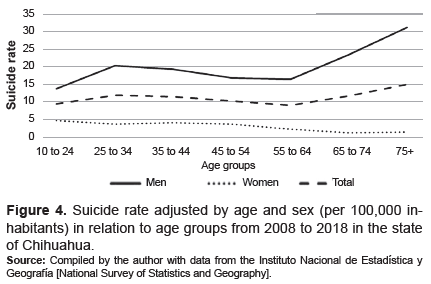
The highest number of completed suicides by age group occurred between the ages of 10 and 24 (n = 1065) and between 25 and 34 (n = 765), and 35 and 44 (n = 649). Table 5 shows the completed suicides and the suicide rate by age group and sex during the study period.
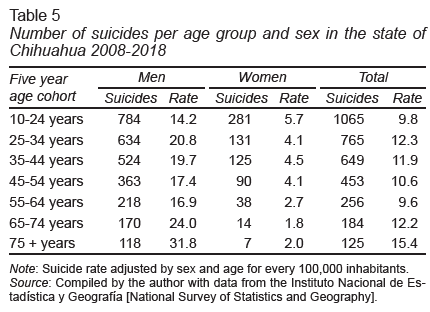
Figure 4 illustrates the association between categorical age and suicide rate. An inverse correlation was found in women with a Spearman correlation coefficient of -.92 (p = .003), while no relationship was found in men or in the two sexes combined (r = .64, p = .119 and r = .36, p = .432, respectively).
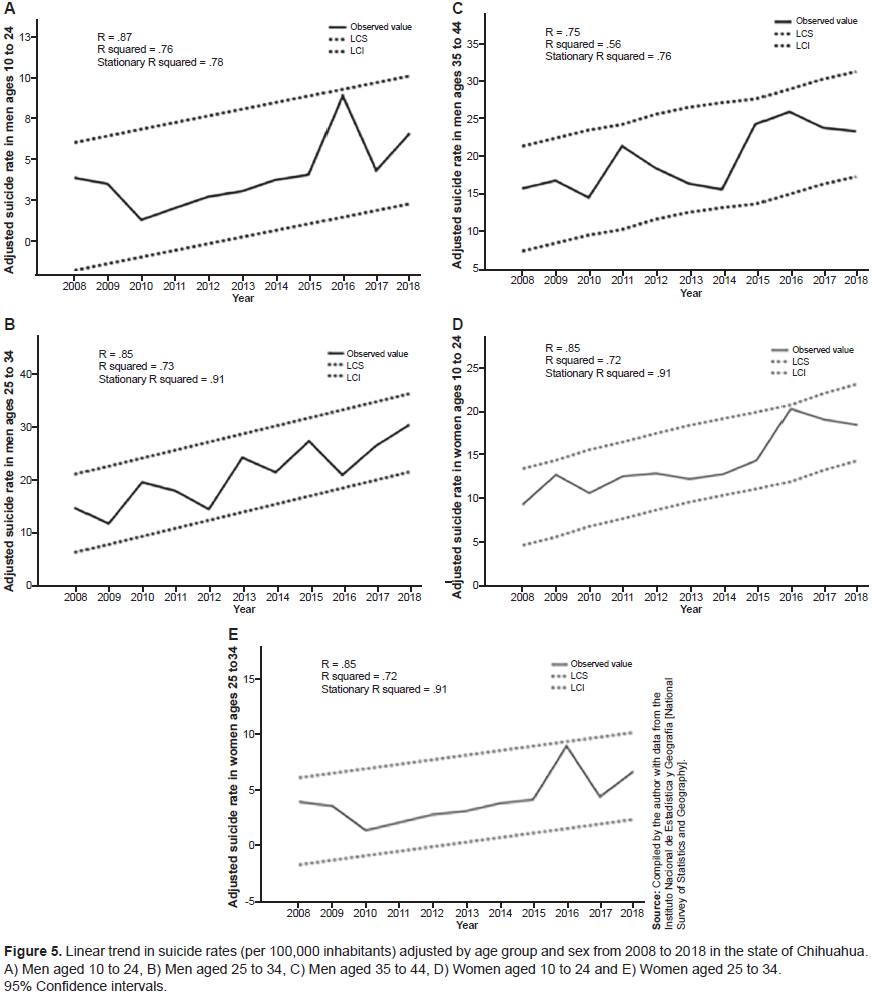
The suicide rate trend was observed in the group aged 10 to 24. Between 2008 and 2018, it increased from 9.3 to 18.5 in men and from 3.6 to 5.1 in women. This increase was evidenced by an R2 value of .76 and .52, respectively (p < .001). In the group aged 25 to 34, a linear increase in suicide rates was also observed in men from 14.7 to 30.4 and in women from 4.0 to 6.7, with an R2 value of .73 and .72 (p < .001), respectively. Finally, in the group aged 35 to 44, the suicide rate for men increased from 15.8 to 23.4, with an R2 of .56 (p < .001). Figure 5 shows the linear relationship of each of these age groups.
Discussion and conclusion
This study is the first to provide information on the behavior of the suicide phenomenon in the state of Chihuahua, where an upward trend in suicide rates was observed from 2008 to 2018, accompanied by the seasonal variation factor, with cyclical peaks during the spring and summer months. This increase in completed suicides in recent years is a phenomenon that has been reported in the literature. In Mexico, Fernández-Niño et al. (2016) found increases in suicide rates for both sexes from 2000 to 2013. This increase is not exclusive to recent years. Borges, Rosovsky, Caballero, and Gómez Castro (2014) observed increases in the suicide rate from 1970 to 1991 for the two sexes combined in Mexico.
This trend has also been accompanied by the seasonal factor. The present article observed that June and July are the months with the highest suicide rates. In fact, this behavior was exponential. From October to March, suicide rates were lower, and began to rise in April. The ambient temperature was associated with this seasonal behavior since temperatures in the summer and winter months are extreme in the state of Chihuahua. These results are consistent with the findings of Fernández-Niño et al. (2016), who found that May was the month with the highest frequency of suicides in Mexico from 2000 to 2013. A recent study analyzed the behavior of suicide in the state of Baja California Sur from 1985 to 2008, observing a sharp increase in suicide rates during the hot season (months with an average temperature of over 30°C), together with an association between temperature and suicide rates (Gaxiola-Robles, Celis de la Rosa, Labrada-Martagón, Díaz-Castro, & Zenteno-Savín, 2013).
A monthly temperature rise of 1°C has been found to be associated with an increase in suicide rates. Between 1968 and 2004, suicide rates in the United States increased by .68% and between 1990 and 2010, they increased by 2.1% in Mexico for each degree centigrade of temperature increase (Burke et al., 2018).
In India, Carleton (2017) reported that with temperatures of 20°C and over, a 1°C increase was associated with a 3.5% increase in suicide rates during the harvest season. Similar results have been obtained in Italy (Muccino et al., 2015) and Canada (Dixon et al., 2014).
In a study undertaken in 29 European countries using a regression analysis with data on completed suicides from 2000 to 2012, Fountoulakis et al. found that climate variables explained 37.6% of the variance in suicide rates in men and 65% when combined with socio-economic variables. Conversely, in women, climate variables alone explained 28.1% of the variance in suicide rates, and 41.7% when socio-economic variables were added (Fountoulakis et al., 2016).
Some studies have attempted to explain the phenomenon of suicide associated with temperature in greater depth. A recent systematic review undertaken on people with suicide attempts in rural areas found that in five studies, summer water shortages were associated with high stress levels and suicide attempts due, for example, to reduced services, lower land values, and unemployment (Crnek-Georgeson, Wilson, & Page, 2017).
Other studies have observed a directly proportional relationship between suicide rates and solar radiation adjusted by geographical area, humidity, temperature (Jee et al., 2017), and air pollution, particularly ozone (O3) and dust (PM10) particles (Casas et al., 2017; Chen & Samet, 2017). PM10 contains large amounts of lipopolysaccharides, which are associated with depression and cytosine expression (Tonelli, Holmes, & Postolache, 2008; Postolache, Manalai, Brenner, & Brundin, 2016). However, since the literature is still limited, it is necessary to continue carrying out and developing these lines of research, addressing mainly neurophysiological factors and studies with qualitative approaches associated with the seasonality of the suicide phenomenon during the spring and summer seasons.
Another relevant finding in this study was the linear increase in suicide rates from 2008 to 2011 in women aged 10 to 34 and in men aged 10 to 44 in the state of Chihuahua, which suggests that this group should be a focus of attention, particularly women, since the group ages 10 to 24 had the highest suicide rates, whereas in men, rates were highest in the group ages 25 to 34 years and 65 years and over. A nationwide study by Borges et al. (2010) in Mexico observed an increase in suicide rates between the ages of 15 and 34 from 1970 to 2007. Women aged 15 to 24 and men aged 20 to 34 and 65 and over recorded the highest suicide rate. These results coincide with the findings of the present study in the state of Chihuahua. They also complement the WHO statement that the prevalence and incidence of suicide in recent decades has represented the second leading cause of death among those ages 15 to 19 (WHO, 2018b).
In the United States, according to the Centers for Disease Control and Prevention (CDC), between 2007 and 2015, suicide rates in women aged 15 to 19 years doubled from 2.4 to 5.1, while suicide rates for 2015 were the highest for the past 40 years (CDC, 2017).
In Mexico, Fadel et al. (2019) observed an increase in suicide rates in the population aged 10 to 14 years from 2000 to 2009 in both sexes, with annual increases of 2.8% in suicide rates from 2005 to 2016. At the same time, Borges et al. (2010) found a 275% increase in suicide rates in the population ages 15 to 29 years between 1970 and 2007. This undoubtedly constitutes a challenge and a public health problem nationwide.
This study also found that suicide prevalence is four times higher in men than women, which coincides with what has been reported in the national literature (Fernández-Niño et al., 2016). However, worldwide, the male-to-female ratio of suicides is 2:1, with an average suicide rate of 13.5 and 7.7 respectively, whereas in the Americas. the suicide rate in men is 15.1 and 4.6 in women, a ratio of 3.3:1 (WHO, 2018a).
One of the main limitations of this study was obtaining suicide data from records in the INEGI database, which may contain errors in the time when deaths were recorded, or the data provided or underreport completed suicides. However, it is one of the main official data sources. To date, no study has been found that evaluates this underreporting and inaccuracies in the information recorded. Another significant limitation of the present study was that average temperatures were obtained at the state rather than the municipal level. However, the statistical analysis performed did not enable us to record temperatures by municipality. This is particularly important in the state of Chihuahua, which has an extremely diverse climate in terms of its regions.
In conclusion, suicide rates in the state of Chihuahua displayed a trend and seasonal variability from 2008 to 2018, with the months of June and July showing the highest suicide rates. This increase has occurred mainly among the young population aged 10 to 34. The seasonal factor of suicide found in this research, together with the high suicide rates, suggest the need to rethink plans and strategies for suicide prevention in the state of Chihuahua. It is important to undertake more studies to analyze the epidemiological behavior of suicide in the state and its relationship with socioeconomic, sociodemographic, sociocultural, and environmental factors, because the evidence is still limited. This would facilitate the identification of the evolution of this phenomenon and the main associated risk factors, to develop more effective prevention and care strategies.